Introduction
Few situations test the depth of human connection like the moment a family member with terminal cancer pushes away a plate of food. For caregivers, providing nourishment represents more than meeting physical needs—it's an act of love, a tangible way to show care when so much feels beyond control. Yet when appetite disappears and a loved one refuses to eat, families face one of the most distressing challenges in terminal cancer care.
Two opposing struggles define this landscape. On one side, families push patients to eat more, driven by the fear that their loved one is starving. On the other, patients with advanced cancer who want to take an active role in their care don't know where to start with nutrition. Both situations require understanding what's happening in the body and what nutrition can—and cannot—accomplish at different disease stages.
What follows covers the physiology, the practical strategies, and the key distinction between comfort nutrition and active nutritional support—so patients and caregivers can make decisions grounded in what's actually happening in the body.
Key Takeaways
- Cancer rewires metabolism so the body can't use nutrients normally; reduced intake is a physiological reality, not failure
- Forcing food causes physical harm (nausea, bloating, aspiration) rather than comfort in terminal patients
- Goals differ by stage: comfort is priority in final weeks; for earlier advanced cancer, nutrition actively supports quality of life
- Small, calorie-dense meals, protein prioritization, and following hunger cues reduce distress for patient and caregiver
- For patients pursuing active management, structured nutritional programs offer targeted support beyond standard palliative care
How Terminal Cancer Changes the Body's Nutritional Needs
Terminal cancer disrupts the body's metabolism. This isn't ordinary hunger or malnutrition — the body's relationship with food changes at a cellular level in ways that conventional nutrition cannot reverse.
Cachexia: The Engine Behind Muscle Wasting
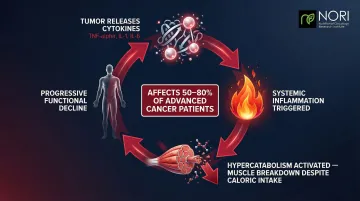
Cancer cachexia is a complex metabolic syndrome marked by severe muscle loss, systemic inflammation, and disrupted energy use. Unlike starvation, it's driven by the tumor's interaction with the body's inflammatory response. Cachexia affects 50–80% of advanced cancer patients and is directly responsible for an estimated 20–30% of all cancer-related deaths.
The mechanism centers on pro-inflammatory cytokines — proteins like TNF-alpha, IL-1, and IL-6 — released by tumors. These trigger hypercatabolism: the body actively breaks down muscle tissue even when calories are being consumed. The condition is defined as muscle loss that "cannot be fully reversed by conventional nutritional support", producing progressive functional decline regardless of dietary intake.
Why Appetite Disappears
Anorexia (loss of appetite) in terminal cancer results from tumor-released compounds, treatment side effects, and natural physiological shutdown—not a choice or sign of giving up. Tumor-released cytokines disrupt hypothalamic pathways that regulate appetite, reducing food-seeking behavior and increasing resting energy expenditure.
Reduced appetite in a terminal patient is not the same as starvation in a healthy person. As the body enters a catabolic state, it produces ketones that can create a sense of comfort and mild euphoria, reducing perceived hunger and thirst. Forcing food can actually prevent this natural ketonemia and prolong the sensation of hunger.
Common treatment-related contributors include:
- Nausea and vomiting
- Mucositis (mouth sores)
- Taste changes (dysgeusia)
- Early satiety (feeling full quickly)
- Fatigue and depression
Some of these are addressable with supportive care, but many represent the body's natural transition as disease advances.
Nutritional Goals in Advanced Cancer: Comfort, Quality of Life, and Beyond
Nutritional goals in advanced cancer exist on a spectrum. Where a patient falls depends on prognosis, performance status, and personal goals of care. The sections below reflect that range — from comfort-focused end-of-life care to active nutritional support for patients still in treatment.
Comfort-Focused Nutrition at End of Life
For patients in the final days or weeks, the goal shifts entirely to symptom relief, eliminating eating-related distress, honoring food preferences, and preserving dignity. Caloric targets and weight maintenance become secondary.
Clinical guidelines from MASCC support clinically assisted nutrition primarily for patients with a prognosis exceeding one month who are at risk of dying from malnutrition before their cancer—not as a universal intervention. A systematic review of end-of-life practices found no study supporting artificial nutrition use in the final week of life.
The ethical dimension runs deep. Families and patients may perceive withholding artificial nutrition as "giving up," but clinical evidence tells a different story.
A 2020 randomized controlled trial found that parenteral nutrition in advanced cancer cachexia improved neither quality of life nor survival — and generated significantly more serious adverse events, mainly infections. Pushing nutrition in the final stage can increase symptom burden without extending life.
Nutrition as Active Support in Advanced (But Not End-Stage) Cancer
The limitations above apply specifically to end-of-life care. Patients with stage III/IV cancer who are still undergoing treatment or actively managing disease occupy a different position on that spectrum — one where nutritional support can improve treatment tolerance, quality of life, and potentially outcomes.
ESPEN guidelines recommend protein intake above 1.0 g/kg/day, and if possible, up to 1.5 g/kg/day for cancer patients. In specific catabolic states, doses up to 2.0 g/kg/day may be required to support positive protein balance.
Specific dietary strategies are active areas of research, though evidence varies in strength:
- Anti-inflammatory dietary patterns linked to reduced systemic inflammation markers
- Omega-3 fatty acid supplementation to support muscle preservation (evidence is mixed but promising)
- Metabolic approaches — such as reduced sugar intake — aimed at exploiting vulnerabilities in cancer cell metabolism

Important limitation: ASCO (2022) states there is "currently insufficient evidence to recommend for or against dietary interventions such as ketogenic or low-carbohydrate diets" to improve outcomes related to quality of life, treatment toxicity, or cancer control.
Practical Nutrition Strategies for Terminal Cancer Patients
Practical nutrition strategies shift depending on whether the patient is in active disease management or transitioning to comfort-only care — but several principles hold across both.
Eating Guidelines for Patients
Prioritize timing and calorie density:
- Eat during times of highest energy in the day
- Choose calorie-dense foods first: healthy fats, protein, dairy, nut butters
- Avoid filling up on low-calorie vegetables or salads when appetite is limited
Keep meals small and easy to manage:
- Small, frequent snacks rather than large meals
- Soft, moist foods requiring minimal chewing: cream soups, yogurt, smoothies, ground meat, soft grains
- Oral nutrition supplements when whole foods are difficult
Approach hydration carefully:
- Offer small, frequent sips rather than large amounts at once
- Moist fruits like watermelon help keep the mouth comfortable
- Caution: Excess fluid intake when kidneys are compromised can worsen swelling or cause lung congestion
Supporting Patients with Swallowing Difficulties
For patients struggling to eat well, swallowing difficulties often compound the challenge. Dysphagia is common in advanced cancer — a SEER-Medicare analysis found a 2-year prevalence of 45% among head and neck cancer survivors, with 9% experiencing aspiration pneumonia.
Practical modifications:
- Texture modifications using standardized frameworks (IDDSI Levels 0-7)
- Positioning recommendations (upright posture, chin-tuck techniques)
- Request instrumental swallowing evaluations when symptoms worsen
Oral care importance:
- Mouth swabs to relieve dryness
- Lip balm for comfort
- Ice chips for moisture
- These small gestures provide real comfort, even when eating is minimal

What Families and Caregivers Need to Know
The most common caregiver fears center on two questions: "Is my loved one starving?" and "Am I failing them by not getting them to eat more?"
At end of life, patients do not experience hunger and thirst the way healthy individuals do. Their reduced intake is a natural part of the body's transition. The ketones produced during this process can actually reduce discomfort.
Follow the Patient's Cues
Offer favorite comfort foods gently. Create a pleasant eating environment with soft music, favorite dishes, and manageable portions. But let the patient decide. Forcing food can cause nausea, bloating, and distress—the opposite of comfort.
Reframe Your Role
At this stage, connection comes from presence — not food. Simple acts can mean more than any meal:
- Sitting quietly together without expectation
- Offering touch, hand-holding, or gentle physical closeness
- Playing favorite music or reading aloud
- Sharing memories or looking through photos
Releasing the pressure around eating gives both patient and caregiver room to focus on what this time is actually for.
When Medically Assisted Nutrition May Be Considered
When oral intake is no longer sufficient, clinicians may consider two forms of medical nutrition support: enteral nutrition (tube feeding directly into the GI tract) or parenteral nutrition (intravenous nutrient delivery). Neither is appropriate for every patient — both carry specific criteria that must be met before they're initiated.
When parenteral nutrition is appropriate:
- Non-functional GI tract (such as inoperable malignant bowel obstruction)
- Prognosis of at least several months
- Performance status that supports the intervention
- Goals of care aligned with life prolongation
Enteral nutrition is preferred when possible due to fewer complications. ESPEN guidelines specify that expected survival should exceed 1-3 months before initiating parenteral nutrition.
That said, these thresholds exist for good reason. For most patients with advanced cancer and cachexia, research has not demonstrated that medically assisted nutrition reverses muscle wasting or significantly prolongs life. It also carries real risks — infection, metabolic complications, and added burden on patients and families. These tradeoffs make the decision highly individual; it's worth discussing your specific goals and prognosis directly with your care team before proceeding.
A Proactive Nutritional Approach for Patients Still Fighting
For advanced cancer patients who have not entered the final end-of-life stage and wish to take an active role in their care, evidence-based nutritional intervention can go beyond palliative support. Emerging approaches target the specific metabolic vulnerabilities of cancer cells.
One such approach involves methionine restriction—a dietary strategy that exploits the elevated methionine dependence of many cancer cells. Cancer cells demonstrate "methionine addiction" and cannot proliferate when this amino acid is restricted, while normal cells remain relatively unaffected. Human clinical data remains limited to early-phase trials, and neither ESPEN nor ASCO currently recommend methionine restriction as standard therapy. It remains an investigational approach that requires proper supervision to implement safely.
For patients who want structured, supervised access to this approach, NORI (Nutritional Oncology Research Institute) has built a home-based nutritional support program around more than 20 years of focused research. The program combines cycled methionine restriction with proprietary nutraceutical combinations and is designed for patients at various stages of advanced cancer.
Key features of the NORI program include:
- Cycled methionine restriction targeting cancer cell metabolic vulnerabilities
- Proprietary nutraceutical combinations developed and manufactured in-house
- Unlimited guidance and support with no clinic visits required
- Free initial consultation for new patients
- Worldwide accessibility for patients pursuing integrative or independent care

Patients actively managing their condition deserve more than a single path forward. To learn whether the NORI program is a fit, call 800-634-3804 or email info@nutritionaloncology.net.
Frequently Asked Questions
Can nutrition reverse cachexia in terminal cancer patients?
Cancer cachexia is driven by tumor-related inflammation and metabolic changes that calories alone cannot reverse. Targeted nutritional strategies may offer modest benefit in earlier disease stages, but not in the final weeks of life.
Is it harmful to force a terminal cancer patient to eat?
Yes. Forcing food on a patient in the final stage of cancer can cause nausea, bloating, aspiration, and discomfort. The dying body produces ketones that reduce hunger and thirst naturally, and the goal should shift to comfort rather than caloric intake.
What foods are best for patients with advanced cancer who are still eating?
Calorie-dense, protein-rich, soft, and easy-to-digest foods work best: smoothies, Greek yogurt, nut butters, cream soups, and oral nutrition supplements. Offer small, frequent portions during the patient's highest-energy hours.
What is the difference between palliative nutrition and therapeutic nutrition in cancer?
Palliative nutrition focuses on comfort, symptom management, and quality of life near end of life. Therapeutic nutrition in advanced cancer aims to actively support the body's ability to manage disease through interventions like anti-inflammatory diets, protein optimization, and nutraceuticals.
When is parenteral nutrition appropriate for a terminal cancer patient?
Parenteral nutrition is generally reserved for patients whose GI tract is non-functional — such as with bowel obstruction — with a prognosis of several months or more and goals of care aligned with life prolongation. It is not recommended as routine care for cachexia or general nutritional decline at end of life.
How can caregivers cope with a loved one who refuses to eat?
This situation is emotionally difficult. Follow the patient's cues, offer small amounts of favorite comfort foods without pressure, and shift the focus of connection from feeding to presence, conversation, and companionship. Your presence matters more than food in these final stages.