Introduction
Radiation therapy for throat cancer creates a painful paradox: treatment targets the very area you need to eat and swallow, at the exact moment your body requires far more calories and protein to repair tissue and fight disease. Up to 80% of head and neck cancer patients experience malnutrition during radiotherapy, and weight loss of just 5% is independently associated with a 1.7 times higher risk of disease-specific mortality.
This article covers why nutrition matters during throat cancer radiation, which foods support healing without aggravating damaged tissue, how to manage the worst side effects through diet, and practical strategies for eating when swallowing becomes painful.
For patients who want support beyond symptom management, NORI offers science-based nutritional programs built around the body's specific needs during cancer care — nutritional support alongside your medical care, not a replacement for it.
Key Takeaways:
- Target at least 30 kcal/kg/day and 1.2–1.5 g/kg/day protein to prevent muscle wasting during radiation
- Avoid high-dose antioxidant supplements — they may reduce treatment effectiveness by protecting cancer cells
- Mucositis peaks around weeks 5–7; use soft, cool, bland foods and salt/baking soda rinses to manage it
- Switch to soft or liquid foods as swallowing worsens; a feeding tube may be necessary if oral intake becomes unsafe
- Expect a slow recovery — side effects commonly persist for weeks to months after treatment ends
Why Nutrition Matters During Throat Cancer Radiation
Malnutrition Affects Up to 80% of Patients During Treatment
The incidence of malnutrition in head and neck cancer patients receiving radiation can reach 80%. Critical weight loss (defined as ≥5% body weight reduction) occurs in 57% of patients during radiotherapy, and severe weight loss (≥10%) affects 26.8% of patients. This isn't just discomfort—it directly impacts survival and healthcare utilization.
Critical weight loss during radiotherapy is independently associated with a 1.7 times higher risk of dying from head and neck cancer. Patients experiencing ≥10% weight loss also face significantly higher rates of unplanned hospital admissions — 51.9% versus 25.3% for those with less weight loss.
Your Body Needs More Fuel to Repair Tissue Damage
Radiation damages healthy tissue alongside cancer cells, and your body requires substantial energy and protein to repair this collateral damage. Protein is the critical foundation for tissue repair, immune function, and muscle mass preservation — especially when appetite is suppressed and eating becomes painful.
Specific nutrients play targeted roles in this process:
- Arginine stimulates lymphocyte function and supports wound healing
- Glutamine acts as a nitrogen donor for healing tissues and is associated with reduced mucosal damage, including mucositis, stomatitis, and pharyngitis
"Eating Well" Looks Different During Radiation
Understanding what the body needs at the nutrient level helps explain why the broader dietary approach changes too. Standard healthy eating guidelines emphasize calorie restriction, whole grains, and lean proteins. During throat radiation, those priorities shift. The goal becomes calorie density rather than restriction — nutrient-rich foods that are soft, moist, and non-irritating take priority over "clean eating" dogma.
For patients navigating these dietary shifts during treatment, NORI's home-based nutritional support program offers personalized diet plans built around the body's specific needs during cancer care. Consultations are available worldwide via phone and Zoom, drawing on over 20 years of focused research in nutritional oncology.
How Radiation Changes Your Nutritional Needs
Eating Ability Deteriorates Over Treatment Course
Radiation's effects on swallowing follow a predictable timeline. Most patients can tolerate normal food textures in weeks 1-3, but the cumulative dose progressively disrupts the mouth and throat lining:
- 15–20 Gy (weeks 1-3): Oral mucositis begins as erythema (redness and inflammation) of the mouth and throat
- ~30 Gy (weeks 3-4): Ulceration develops, making swallowing increasingly painful
- 60–72 Gy (weeks 5-7): Peak severity — thick mucus, severe mouth sores, and dysphagia are common
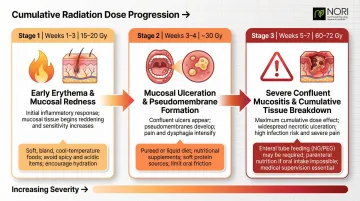
This progression forces dietary transitions. Mouth sores, painful swallowing, dry mouth, and thick mucus make soft or liquid diets necessary by weeks 4-6 for most patients.
Clinical Guidelines Mandate Aggressive Macronutrient Targets
Radiation drastically increases metabolic demands. Authoritative guidelines specify elevated targets to prevent muscle wasting:
Energy and Protein Targets:
- At least 30 kcal/kg/day in energy (per ASPEN and UK National Guidelines)
- 1.2–1.5 g/kg/day in protein (per ASPEN and ESPEN 2021)
- Adequate caloric intake ensures protein goes toward muscle preservation — not fuel
Practical calculation: A 70 kg (154 lb) patient should target:
- 2,100 calories per day minimum
- 84-105 grams of protein per day
These targets are aggressive for a reason — meeting them from the onset of treatment is essential for maintaining weight and functional status.
The Antioxidant Paradox: When "Healthy" Supplements Backfire
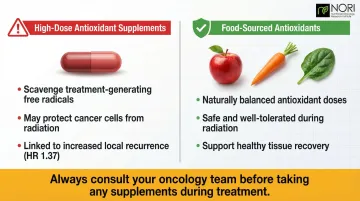
While hitting calorie and protein targets is critical, what you avoid during treatment matters just as much. Many patients turn to antioxidant supplements (Vitamins A, C, E, beta-carotene) hoping to reduce treatment toxicity — but clinical evidence strongly advises against this during radiation therapy.
Why antioxidants are contraindicated:
- Radiation kills cancer cells by generating free radicals and oxidative damage
- Antioxidants scavenge these free radicals, potentially protecting cancer cells alongside normal tissue
- A randomized trial of 540 head and neck cancer patients found that high-dose alpha-tocopherol (400 IU/day) and beta-carotene (30 mg/day) supplementation during radiation increased local recurrence rates (HR 1.37)
American Cancer Society guidance: Cancer patients receiving radiation should obtain antioxidants through food sources and avoid dietary supplements exceeding 100% of the Daily Value. Discuss all supplements with your oncology team before continuing during treatment.
Best Foods to Eat During Throat Cancer Radiation Treatment
High-Quality Protein Sources That Are Soft and Easy to Swallow
Protein at every meal matters for muscle preservation. Choose options that slide down easily:
- Scrambled or soft-boiled eggs – tender texture, complete protein
- Greek yogurt and cottage cheese – high protein density, cool and soothing
- Soft-cooked fish – salmon, cod, tilapia flake easily and provide omega-3 fatty acids
- Nut butters blended into smoothies – calorie-dense, no chewing required
- Silken tofu – neutral flavor, soft texture, versatile base
- Well-cooked beans – mashed or pureed for easier swallowing
Soft, Nutrient-Dense Carbohydrates as Calorie Vehicles
Carbohydrate sources serve dual purposes: providing energy and acting as vehicles for adding healthy fats to boost calorie density.
Recommended options:
- Oatmeal cooked in whole milk (not water)
- Mashed sweet potatoes with olive oil or butter
- Soft-cooked pasta with cream-based sauces
- Cream of wheat or cream of rice
- Well-cooked white or brown rice
Calorie-boosting strategy: Add 1-2 tablespoons of olive oil, butter, or avocado to each serving. This adds 100-200 calories without requiring extra chewing or swallowing effort.
Nutritional Shakes: Essential in Later Treatment Weeks
When oral food intake becomes insufficient to meet the 30 kcal/kg/day target, oral nutritional supplements (ONS) become critical.
Clinical research backs this approach. One randomized controlled trial found that patients receiving counseling plus ONS lost significantly less weight (an average of 1.6 kg less) than those receiving counseling alone. ONS also reduced the likelihood of treatment interruptions by 60%, meaning patients were more likely to stay on schedule with their radiation plan.
Options include:
- Commercial supplements: High-calorie protein shakes (Ensure Plus, Boost VHC, Orgain)
- Homemade versions: Whole milk or plant-based milk + protein powder + banana + nut butter + avocado (blend until smooth)
Aim for 2-3 shakes per day if solid food intake drops below target.
Hydration-Supporting Foods and Fluid Targets
Maintaining hydration becomes increasingly difficult as saliva production decreases. Salivary flow typically drops 50-60% within the first week of radiation, with some partial recovery to around a 20% reduction by week 7.
Target: 8-12 cups (2-3 liters) of fluid per day
Hydration sources:
- Broths and mild soups (not tomato-based)
- Non-acidic fruit nectars (pear, peach, apricot—not citrus)
- Gelatin-based foods and popsicles
- Watermelon and other high-water-content fruits
- Herbal teas (cooled or room temperature)
All non-alcoholic, non-caffeinated beverages count toward your fluid target.
Foods and Substances to Avoid During Radiation
Acidic Foods Irritate Inflamed Tissue
Acidic foods and beverages directly irritate the inflamed mucosal lining of your throat, worsening pain and mouth sores.
Strict avoidance list:
- Citrus fruits and juices (oranges, grapefruits, lemons, limes)
- Tomato-based sauces and soups
- Vinegar and vinegar-based dressings
- Carbonated beverages (the carbonation itself irritates)
Mechanical Irritants: Rough, Crunchy, or Dry Textures
Damaged throat tissue cannot tolerate foods that scrape, stick, or require extensive chewing.
Foods to eliminate:
- Toast, crackers, chips, pretzels
- Dry bread or baked goods
- Raw vegetables (carrots, celery, broccoli)
- Nuts and seeds in whole form
- Granola and dry cereals
Heat and spice create a separate category of irritation. Even if a food has a soft texture, it can still aggravate inflamed tissue if it's too hot or heavily seasoned:
- Spicy foods (chili peppers, hot sauce, curry)
- Foods served steaming hot — always allow to cool to room temperature first
Alcohol and Caffeine Worsen Dry Mouth
Alcohol and caffeinated beverages act as drying agents, worsening xerostomia (dry mouth), which is among the most persistent radiation side effects.
- Avoid alcohol completely during treatment — it inflames throat tissue, impairs wound healing, and contributes to neck fibrosis after radiation
- Limit coffee and black tea to 1-2 cups per day; choose decaffeinated versions or herbal teas when possible
- Skip commercial mouthwashes that contain alcohol, as these worsen dryness further
Limit Processed Foods (But Not for Typical Reasons)
During radiation, processed foods are a problem because they crowd out the nutrient-dense options your body needs to repair tissue and maintain weight.
Minimize:
- Refined sugars and sweets that crowd out protein-rich foods
- Excessive added salt (can irritate sores)
- Ultra-processed convenience foods with minimal nutritional benefit
Managing Radiation Side Effects Through Diet
Mouth Sores and Mucositis
Mucositis ranks among the most debilitating side effects for throat radiation patients. A systematic review found a mean incidence of 80%, with 56% of patients receiving altered fractionation radiation experiencing severe (WHO Grade 3-4) mucositis. Grade 3 involves ulcers that require a liquid-only diet; Grade 4 means eating or drinking becomes impossible without medical intervention.
Choose soft, bland, cool or room-temperature foods:
- Puddings and custards
- Plain gelatin
- Yogurt (unflavored or vanilla)
- Ripe mashed banana
- Applesauce (unsweetened)
- Smooth nut butters (thinned with liquid)
- Soft-scrambled eggs
- Well-cooked oatmeal
Oral care protocol: Memorial Sloan Kettering Cancer Center recommends rinsing the mouth every 4 to 6 hours with a solution of 1 quart (4 cups) of water mixed with 1 teaspoon of salt and 1 teaspoon of baking soda. This bland rinse reduces bacteria and promotes healing. Do not use chlorhexidine mouthwashes—research does not support their use for radiation-induced mucositis.
Consistently avoiding irritants — acidic, spicy, and rough-textured foods — alongside excellent oral hygiene is the most effective way to reduce mucositis severity.
Dry Mouth and Thick Mucus
Xerostomia (dry mouth) and thick, sticky mucus are nearly universal during throat radiation.
For dry mouth:
- Carry water everywhere and sip frequently throughout the day
- Add gravies, sauces, and oils to all solid foods
- Choose naturally moist foods: watermelon, yogurt, soup, smoothies
- Try sugar-free mints or chewing gum to stimulate saliva production
- Consider mucin-based saliva substitutes (available over the counter) for symptomatic relief
For thick mucus:
- Sip warm water or warm herbal tea with honey throughout the day
- Stay well-hydrated (adequate fluid intake thins secretions)
- Fresh pineapple contains bromelain, an enzyme that breaks down proteins in thickened saliva—though patients with active mouth ulcers should avoid it due to stinging
Taste Changes and Loss of Appetite
Dysgeusia (taste alteration) affects up to 70% of oral cancer patients during treatment.
Managing metallic or altered tastes:
- Use plastic or bamboo utensils instead of metal
- Eat foods cold or at room temperature (less aroma, better tolerance)
- Experiment with mild herbs and seasonings (avoid these if mouth sores are present)
- Small amounts of honey or maple syrup can enhance palatability
When appetite fades, structure matters more than hunger cues. Try these strategies:
- Eat on a schedule every 2-3 hours rather than waiting to feel hungry
- Choose small portions 5-6 times per day instead of 3 large meals
- Eat in a comfortable, low-stress environment
- Keep calorie-dense snacks within easy reach
Practical Eating Strategies When Swallowing Is Difficult
Transition Through Food Textures as Swallowing Worsens
When texture modification becomes necessary to prevent aspiration, follow this progression:
IDDSI Framework (International Dysphagia Diet Standardisation Initiative):
- Level 6 — Soft & Bite-Sized: tender pieces (≤1.5cm), mashed easily with a fork
- Level 5 — Minced & Moist: soft with small lumps (≤4mm), minimal chewing required
- Level 4 — Pureed: completely smooth, no chewing needed

Work with a speech-language pathologist to identify which textures are safe for your specific anatomy. Doing swallowing exercises during chemoradiotherapy significantly reduces muscle deterioration and supports long-term swallowing function.
Batch-Prep Strategies for Efficiency
Managing textures is easier when food is ready before fatigue sets in. Preparing meals in advance — ideally before treatment begins — reduces the daily effort of eating when energy is lowest.
Recommended approach:
- Prepare and freeze soft, calorie-dense meals: soups, stews, smoothie packs, mashed dishes
- Portion into single-serving containers
- Label with date and calorie/protein content
- Keep a simple food and fluid log to monitor whether you're meeting targets
Watch your weight: Track it every 3-5 days. If you're losing weight despite these efforts, contact your care team immediately.
Feeding Tube Placement: A Supportive Tool, Not a Failure
When oral intake cannot meet the 30 kcal/kg/day requirement despite all strategies, enteral feeding may be necessary.
NCCN guidelines strongly consider prophylactic PEG tube placement for patients with:
- Severe weight loss prior to treatment (5% past 1 month, or 10% past 6 months)
- Ongoing dehydration
- Severe dysphagia
- Large fields of high-dose radiation to the mucosa anticipated
PEG placement reduces malnutrition risk and prevents treatment interruptions when swallowing becomes unsafe. One randomized trial found that only 18-29% of patients remained PEG-dependent at 6 months post-treatment, meaning most successfully return to oral feeding over time.
Nutrition After Radiation Ends: Recovery and Long-Term Health
Side Effects Persist Long After Final Treatment Session
Recovery is gradual, not immediate. Dry mouth, sore throat, and swallowing difficulty often continue for weeks to months.
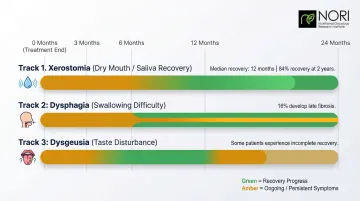
Timeline for recovery:
- Xerostomia: Median salivary recovery time is 12 months, with cumulative recovery rates reaching 84% at two years
- Dysphagia: While acute dysphagia resolves for many within 6 months, 16% of patients develop new-onset dysphagia more than 6 months after treatment due to radiation-induced fibrosis
- Dysgeusia: Taste sensation usually recovers within 3-12 months, though some patients experience incomplete recovery
Dietary guidance: Continue soft or liquid diets and nutritional supplements until swallowing normalizes. Gradually reintroduce textures as tolerated—do not rush this process.
Transition to Plant-Rich, Anti-Inflammatory Diet for Survivorship
Long-term diet quality directly impacts survival outcomes. A prospective cohort study of 468 head and neck cancer patients found that each 11-point increase in adherence to the Alternative Healthy Eating Index (AHEI-2010) was associated with a 60% decrease in all-cause mortality risk. That same study found nutrient-dense diet adherents were 93% less likely to die during the first three years after diagnosis.
Recommended long-term dietary pattern:
- Emphasize vegetables, fruits, and whole grains
- Choose lean proteins (fish, poultry, legumes)
- Limit red meat and processed meats
- Avoid alcohol — survivors who drink do not live as long as those who abstain
- Minimize sugar-sweetened beverages and refined sugars
- Include healthy fats (olive oil, avocado, nuts)
For patients seeking structured nutritional support during this transition, NORI (Nutritional Oncology Research Institute) provides home-based programs tailored to the long-term dietary needs of cancer survivors. Call 800-634-3804 or email info@nutritionaloncology.net for a free initial consultation.
Work with a Registered Oncology Dietitian
Nutritional support shouldn't end when radiation does. A registered oncology dietitian can complement any structured program by adjusting your plan as healing progresses and flagging early warning signs.
Practical steps for post-treatment follow-up:
- Schedule dietitian check-ins at 1 month, 3 months, and 6 months post-treatment
- Track your weight every 3-5 days and report any sudden drops to your care team
- Keep a symptom log noting changes in swallowing, taste, or appetite between visits
- Ask your dietitian to reassess your supplement needs as whole-food tolerance improves
Frequently Asked Questions
What foods should you avoid with throat cancer?
Avoid acidic foods (citrus, tomatoes), rough or dry-textured foods (toast, crackers, chips, raw vegetables), spicy foods, and alcohol. These aggravate throat irritation, worsen mouth sores, and interfere with tissue healing during and after radiation treatment.
What is the best diet when having radiotherapy?
The best diet is high in calories (at least 30 kcal/kg/day) and protein (1.2–1.5 g/kg/day), with soft or liquid textures as swallowing becomes difficult. Focus on nutrient-dense whole foods and calorie-dense additions like oils and nut butters to preserve weight and muscle mass throughout treatment.
What foods are good for mouth sores?
Soft, cool, bland foods provide relief: yogurt, applesauce, mashed bananas, smooth nut butters (thinned with liquid), soft-cooked oatmeal, plain gelatin, pudding, and cold or room-temperature broths. Avoid hot, spicy, acidic, or rough-textured foods.
What is the fastest way to cure mucositis?
Mucositis management combines dietary changes (soft, non-irritating foods), consistent salt-and-baking-soda mouth rinses (1 tsp each in 1 quart water, 4–6 times daily), excellent oral hygiene, and medical treatments prescribed by your care team. Diet alone won't resolve it, but it meaningfully reduces severity alongside proper oral care.
Do and don'ts after radiotherapy?
Do continue soft/liquid diets until swallowing heals; do track weight every 3-5 days; do gradually reintroduce textures as tolerated. Don't rush back to normal eating before your throat heals; don't stop nutritional supplements until weight and strength are restored; don't ignore persistent swallowing difficulties; report them to your care team promptly.
Why do they remove teeth before radiotherapy?
Radiation reduces blood supply to the jaw bone, sharply increasing the risk of osteoradionecrosis (bone death). If an infected or damaged tooth requires extraction after radiation, the bone often cannot heal — causing severe, hard-to-treat complications. Removing compromised teeth at least 2 weeks beforehand allows gums to heal and protects long-term oral health.