Introduction
Esophageal cancer presents one of the most severe nutritional challenges in oncology. Difficulty swallowing is often the first symptom, and it arrives early enough that 76% of esophageal cancer patients are already malnourished at diagnosis — a rate far higher than most other cancers. That malnutrition directly drives higher surgical complication rates, longer hospital stays, and reduced therapy effectiveness. Addressing it isn't optional; it's central to treatment success.
This guide covers the full picture of nutritional management for esophageal cancer patients:
- What to eat and what to avoid at each treatment stage
- Evidence-based strategies for eating when swallowing is difficult
- How to prevent malnutrition from undermining your treatment outcomes
Key Takeaways
- Malnutrition affects 76% of esophageal cancer patients at diagnosis—early intervention is essential for treatment success
- Focus on soft, high-calorie, high-protein foods like Greek yogurt, pureed legumes, eggs, and flaky fish
- A 10 g/day increase in dietary fiber reduces esophageal cancer risk by 31%—dark leafy greens and berries are strong sources
- Avoid hard textures, acidic/spicy foods, alcohol, processed meats, and added sugars—high sugar intake raises EAC risk by 62%
- Post-surgery: eat small frequent meals, separate liquids from solids, and adjust diet to manage dumping syndrome
Why Malnutrition Is a Major Risk in Esophageal Cancer
Malnutrition in esophageal cancer stems from multiple compounding sources, each one eroding nutritional status from a different angle.
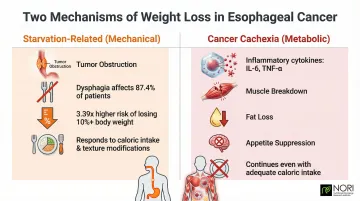
Two Types of Weight Loss:
Starvation-Related (Mechanical): Dysphagia affects 87.4% of patients, with those experiencing swallowing difficulty facing a 3.39 times higher risk of losing more than 10% of their body weight. The tumor physically obstructs food passage, reducing intake regardless of appetite.
Cancer Cachexia (Metabolic): Inflammatory cytokines—specifically IL-6 and TNF-α—actively break down muscle tissue, accelerate fat loss, and suppress appetite through hypothalamic signaling. This process continues even when caloric intake is adequate.
Clinical Consequences Are Severe:
Malnourished patients face dramatically worse outcomes. A 2026* prospective study found malnourished patients had a 2.74 times higher mortality risk compared to well-nourished patients. Surgical complications increase sharply—GLIM-defined malnutrition multiplies total postoperative complication risk by 7.52.
These risks make the starvation/cachexia distinction clinically meaningful — each requires a different response. Starvation responds well to increased caloric intake and texture modifications. Cachexia demands strategies focused on preserving lean muscle mass, including adequate protein intake (1.2–1.5 g/kg/day) and targeted nutritional support.
Best Foods for Esophageal Cancer Patients
High-Protein, Soft-Textured Options
Protein supports tissue repair, immune function, and muscle preservation during treatment. ASPEN guidelines recommend 1.2–1.5 g/kg/day for esophageal cancer patients undergoing treatment.
Top protein sources:
- Greek yogurt and cottage cheese (smooth, easy to swallow, 15-20g protein per serving)
- Eggs (soft scrambled or poached)
- Flaky fish like salmon or tuna (tender, omega-3 rich)
- Ground or tender chicken/turkey with gravy
- Smooth nut butters (almond, peanut, cashew)
- Pureed or mashed legumes (beans, lentils, chickpeas)
- Soft tofu blended into smoothies
High-Calorie Healthy Fats
When swallowing is difficult, calorie-dense fats help maintain weight without requiring large volumes or extensive chewing.
- Avocado (blend into smoothies or mash onto soft bread)
- Olive oil drizzled over pureed vegetables
- Nut butters mixed into oatmeal or yogurt
- Full-fat dairy products
- Coconut oil in cooking
Plant Foods with Anti-Cancer Research Support
Observational studies link specific plant foods with reduced esophageal cancer risk.
Dietary fiber: A 10 g/day increase in fiber intake reduces esophageal cancer risk by 31%. Soft fiber sources include oatmeal, brown rice cooked tender, pureed legumes, and cooked fruits like applesauce or pear compote.
Dark leafy greens: The NIH-AARP study found high spinach intake reduced esophageal adenocarcinoma risk by 34%. Blend spinach into smoothies or puree cooked greens into soups.
Berries: Black raspberries specifically reduced oxidative stress markers in Barrett's esophagus patients in a Phase I clinical trial. Blend fresh or frozen berries into smoothies.
Cruciferous vegetables: Cabbage and broccoli contain protective compounds; steam until very soft or puree into soups.
Patients seeking more targeted dietary strategies—such as methionine restriction combined with nutraceutical support—may benefit from working with a nutritional oncology program like NORI, which offers free initial consultations. These micronutrients below also show meaningful research support for esophageal cancer specifically.
Key Micronutrients
Research links specific nutrients with reduced esophageal cancer risk:
- Vitamin C: Each 50 mg/day increase reduces risk by 13%. Sources: cooked sweet potato, berries, citrus when tolerated.
- Beta-carotene: Found in carrots, sweet potato, winter squash (cook soft and mash).
- Selenium: Brazil nuts, fish (2-3 Brazil nuts daily provide adequate selenium).
- Folate: Leafy greens, legumes, fortified grains.
Foods and Substances to Avoid
Foods That Worsen Dysphagia and Irritate Tissue
Avoid anything that makes swallowing more difficult or painful:
- Hard, dry, or sharp textures: chips, crackers, crusty bread, tough cuts of meat
- Extremely hot or cold foods/beverages
- Acidic foods: citrus juice, tomato sauce, vinegar-heavy dressings
- Spicy foods (worsen mucositis during radiation)
Dietary Risk Factors Linked to Disease Progression
Added sugars: Patients in the highest quintile of added sugar intake faced a 62% greater risk of esophageal adenocarcinoma than those in the lowest, per the NIH-AARP study. Limit sweetened beverages, desserts, and processed foods with added sugars.
Alcohol: Heavy drinking increases esophageal squamous cell carcinoma risk nearly 5-fold. Complete avoidance is recommended during treatment.
Red and processed meats: Limit bacon, sausage, deli meats, and red meat portions — meta-analyses link high intake to elevated esophageal adenocarcinoma risk, with processed meats showing an RR of 1.41 and red meat an RR of 1.31 in case-control studies.
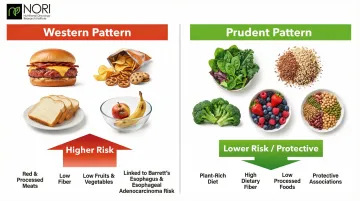
The Western Dietary Pattern
Diets high in red meat, processed foods, and low in fruits and vegetables increase Barrett's esophagus and esophageal adenocarcinoma risk. Multiple studies point to a clear contrast between two eating patterns:
- Western pattern (red meat, processed foods, low fiber) — associated with higher Barrett's esophagus and esophageal adenocarcinoma risk
- Prudent pattern (plant-rich, high-fiber, low in processed foods) — shows protective associations across multiple studies
Phase-by-Phase Nutrition Guide: Before, During, and After Treatment
Before Treatment Begins
The pre-treatment window is critical. Start optimizing nutrition before chemotherapy, radiation, or surgery begins.
Key actions:
- Build or maintain weight and lean muscle mass while intake is still manageable
- Emphasize high-calorie, high-protein foods if swallowing allows
- Request early referral to a registered dietitian specializing in oncology
- Begin exploring texture-modified foods if dysphagia is already present
During Chemotherapy and Radiation Therapy
Chemo and radiation create overlapping side effects: mucositis, dry mouth, taste changes, nausea, and progressive dysphagia.
Dietary response strategies:
- Shift to soft and pureed foods as tolerated
- Eat 6-8 small meals daily instead of 3 large ones
- Use high-calorie/high-protein liquid supplements between meals (Ensure Plus, Boost VHC, or homemade smoothies with protein powder, nut butter, and fruit)
- Stay hydrated with 8+ cups of fluid daily (sip throughout the day if large amounts are difficult)
- If oral intake becomes insufficient, a feeding tube (nasogastric or jejunostomy) may be medically indicated. It's a practical measure to preserve nutrition while the body heals — not a sign of treatment failure.
After Esophagectomy (Surgery)
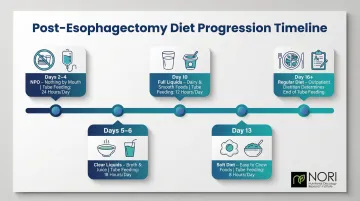
Post-surgical diet progression follows a strict timeline to protect the healing anastomosis:
| Timeline | Diet Phase | Tube Feeding Support |
|---|---|---|
| Days 2-4 | Nothing by mouth (NPO) | 24 hours/day |
| Days 5-6 | Clear liquids (broth, clear juice) | 18 hours/day |
| Day 10 | Full liquids (thicker liquids, dairy) | 12 hours/day |
| Day 13 | Soft diet (minimal chewing) | 8 hours/day |
| Day 16+ | Regular diet (surgeon-determined) | Outpatient dietitian determines when to stop |
Long-term post-surgical changes:
Your stomach is repositioned into your chest, significantly limiting capacity. Permanent adaptations include:
- Eat 6+ small meals daily (never 3 large meals)
- Chew thoroughly and eat slowly
- Separate liquids from solids: drink 30-60 minutes before or after meals, not during
- Sleep with the head elevated 30 degrees or higher — the lower esophageal sphincter is removed during surgery, leaving the stomach highly prone to reflux without positional support
Practical Strategies to Eat Well Despite Symptoms
Managing Dysphagia (Difficulty Swallowing)
Texture modifications:
- Choose soft, moist, or pureed textures
- Add gravies, sauces, broths, or healthy oils to dry foods
- Keep a blender or food processor accessible
- Start with 4 oz portions of liquids and advance gradually
Professional support: Work with a Speech-Language Pathologist for severe swallowing dysfunction. SLPs provide swallowing exercises, texture recommendations, and compensatory strategies to reduce aspiration risk.
Preventing Dumping Syndrome Post-Surgery
Dumping syndrome occurs when stomach contents empty too rapidly into the small intestine, causing cramping, diarrhea, and sweating within 10-30 minutes (early dumping) or reactive hypoglycemia 1-3 hours later (late dumping).
Prevention strategies:
- Limit added sugars and simple carbohydrates
- Eat small portions (4-6 oz per meal)
- Separate liquids from solids (wait 30-60 minutes)
- Choose complex carbohydrates over refined options
- Avoid carbonated beverages
Managing Acid Reflux Post-Esophagectomy
Without the lower esophageal sphincter, reflux is guaranteed unless you follow strict postural rules.
Essential habits:
- Sit upright for 60-90 minutes after all meals
- Eat the last meal at least 2 hours before bedtime
- Sleep with head elevated at 30-degree angle using a wedge pillow
- Wear loose-fitting clothing around the abdomen
- Avoid carbonated beverages and large fluid volumes at once
These self-management strategies address the most common post-treatment challenges, but some patients need more individualized guidance — especially when symptoms overlap or nutritional deficits compound. NORI's home-based nutritional support program offers personalized protocols and ongoing support for esophageal cancer patients, with a free initial consultation available to those who want to explore integrative nutritional approaches alongside their care plan.
Frequently Asked Questions
What is the best diet for someone with esophageal cancer?
A high-calorie, high-protein, soft or pureed plant-rich diet is recommended. Prioritize foods like Greek yogurt, pureed legumes, soft-cooked vegetables, eggs, flaky fish, and smoothies — while limiting red and processed meats, alcohol, and added sugars. Aim for 10+ grams of dietary fiber daily; dark leafy greens in particular show protective associations in research.
What foods should esophageal cancer patients avoid?
Avoid hard, dry, or sharp-textured foods (chips, crackers, tough meat), acidic and spicy foods, alcohol, processed and red meats, added sugars, and extremely hot or cold beverages. These foods worsen symptoms like dysphagia and mucositis or are linked to disease progression in research.
How do you manage difficulty swallowing during esophageal cancer care?
Stick to pureed and soft-textured foods, and add gravies, broths, or sauces to all meals. Eat slowly in small portions, and work with a dietitian or Speech-Language Pathologist for a personalized swallowing assessment. Feeding tubes may be medically necessary if oral intake becomes insufficient.
What is dumping syndrome and how can diet help prevent it?
Dumping syndrome is the rapid emptying of stomach contents into the small intestine after esophagectomy, triggered by high-sugar or high-volume meals. It causes cramping, diarrhea, sweating, and reactive hypoglycemia. Manage it by eating small frequent meals, limiting added sugars, and separating liquids from solids by 30-60 minutes.
Can diet affect esophageal cancer outcomes beyond just managing symptoms?
Yes. Research shows dietary patterns rich in plants, fiber, and micronutrients (while low in red/processed meats) are associated with reduced risk of Barrett's esophagus and esophageal adenocarcinoma progression. Better nutritional status is linked to improved treatment tolerance, fewer surgical complications, and better recovery outcomes.
When can esophageal cancer patients return to a normal diet after surgery?
Diet progresses gradually from clear liquids (days 5-6) to full liquids (day 10) to soft foods (day 13) over the first 2-3 weeks post-surgery. Most patients adapt to small, frequent regular-textured meals over several months. Some adjustments — including smaller portions and separating liquids from solids — remain permanent due to altered stomach anatomy.