Introduction
Pancreatic cancer carries one of the bleakest prognoses in oncology. With a 13.3% overall 5-year survival rate and over 50% of patients diagnosed after the disease has already spread, conventional treatment alone often falls short. Only about 20% of newly diagnosed patients qualify for surgery—the sole potentially curative option—leaving most to navigate chemotherapy resistance, progressive disease, and limited survival windows.
That reality has pushed patients and caregivers to look beyond the standard three-option framework. Holistic treatment for pancreatic cancer doesn't mean rejecting conventional oncology — it means building a wider toolkit that addresses the disease from multiple angles at once.
In this context, holistic treatment means combining evidence-informed approaches with — or in some cases, as an alternative to — conventional care:
- Nutritional strategies that alter the metabolic environment cancer cells depend on
- Natural compounds with documented activity against tumor growth
- Mind-body practices that reduce treatment side effects and improve resilience
- Lifestyle interventions that support the body's own defenses and reduce toxicity
This guide walks through each of these areas with specific, research-grounded detail — and explains how to combine them into a coherent, personalized care plan.
Key Takeaways
- Pancreatic cancer's 13.3% five-year survival rate reflects late diagnosis, aggressive biology, and chemotherapy resistance
- Holistic approaches target cancer cell vulnerabilities that standard treatment often misses
- Nutritional strategies targeting cancer cells' methionine dependency show strong evidence and integrate safely with standard care
- Natural compounds like curcumin, vitamin E tocotrienols, and sodium selenite show wellness-supporting effects in preclinical and early clinical research
- Gentle exercise, stress reduction, and adequate sleep improve treatment tolerance, reduce inflammation, and support quality of life
- Coordinate with an integrative oncology team before adding supplements or dietary protocols — interactions can be harmful
Why Pancreatic Cancer Demands More Than Conventional Treatment Alone
Pancreatic ductal adenocarcinoma (PDAC) presents unique biological challenges that severely limit treatment effectiveness. The tumor microenvironment is exceptionally dense, with cancer-associated fibroblasts producing thick extracellular matrix that collapses blood vessels and prevents chemotherapy drugs from reaching cancer cells. This physical barrier, combined with late-stage presentation in most cases, creates a treatment-resistant disease.
Current statistics paint a sobering picture: only 13.3% of pancreatic cancer patients survive five years, with stage IV (distant metastasis) survival plummeting to just 3.2%. Approximately 51% of patients are diagnosed when cancer has already spread beyond the pancreas, eliminating surgical options for the majority.
Gemcitabine resistance represents the central obstacle in chemotherapy. Cancer cells develop resistance through multiple mechanisms: downregulating nucleoside transporters (particularly hENT1) that bring the drug into cells, reducing deoxycytidine kinase enzymes that activate it, and increasing cytidine deaminase that breaks it down.
The tumor environment compounds this further. Cancer-associated fibroblasts and immune cells release deoxycytidine that directly competes with gemcitabine for cellular uptake, creating a hostile chemical environment that neutralizes treatment before it reaches its target.
Oncologists and researchers increasingly recognize that conventional treatment alone cannot address the full scope of pancreatic cancer's biology. Two distinct but overlapping paths exist for patients exploring broader options:
- Complementary approaches: Evidence-based interventions used alongside chemotherapy and radiation to enhance effectiveness and reduce side effects
- Alternative approaches: Evidence-informed protocols used instead of conventional treatment when patients choose a different path or have exhausted standard options
Holistic strategies deliver the most benefit when they are evidence-informed, professionally supervised, and integrated with full informed consent — whether used alongside conventional care or, in specific circumstances, as the primary approach.
Nutritional and Dietary Strategies as Holistic Cancer Support
The Pancreas Crisis: Why Nutrition Is Non-Negotiable
The pancreas performs two critical functions: producing digestive enzymes (exocrine function) and regulating blood sugar through insulin and glucagon (endocrine function). Pancreatic cancer disrupts both. Pancreatic exocrine insufficiency (PEI) affects 72% of advanced PDAC patients, causing severe maldigestion and fat malabsorption. This creates critical deficiencies in fat-soluble vitamins A, D, E, and K—leading to bone loss, neuropathy, bleeding disorders, and immune dysfunction.
Compounding this, cancer cachexia affects approximately 80% of pancreatic cancer patients—a wasting syndrome marked by muscle loss, appetite suppression, and metabolic dysfunction. Cachexia directly reduces survival, increases chemotherapy side effects, and predicts early treatment failure. For pancreatic cancer patients, nutrition isn't optional—it's survival-critical.
Anti-Inflammatory, Nutrient-Dense Eating Patterns
The foundation of holistic nutritional support emphasizes whole foods that reduce inflammation and provide bioavailable nutrients:
- Lean proteins: Fish (especially omega-3-rich salmon and sardines), poultry, plant proteins (legumes, tofu)
- Healthy fats: Avocado, olive oil, nuts, seeds (contrary to myth, healthy fats are essential—not forbidden—for pancreatic patients)
- Colorful vegetables and fruits: Cruciferous vegetables (broccoli, cauliflower), leafy greens, berries, citrus
- Whole grains: Quinoa, brown rice, oats (in moderate amounts)
- Limit: Processed foods, refined sugars, red meat, alcohol
Debunking the fat myth: Many patients wrongly believe all fat must be avoided. While pancreatic insufficiency impairs fat digestion, healthy fats remain essential for nutrient absorption, hormone production, and cellular function. The solution is enzyme replacement therapy (discussed below) combined with moderate, high-quality fat intake—not fat elimination.
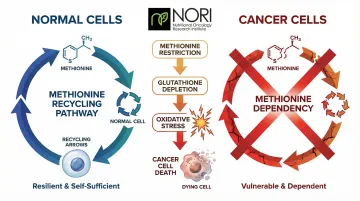
Methionine Restriction: Exploiting a Cancer Cell's Nutritional Dependency
Cancer cells exhibit a unique metabolic dependency: they cannot survive without external methionine, an essential amino acid. Normal cells can recycle methionine through alternative biochemical pathways, but all cancer cells are "methionine-addicted"—requiring constant dietary supply to maintain growth and division.
This dependency creates a therapeutic opening. Methionine restriction depletes cancer cells' ability to synthesize glutathione — the molecule they depend on to maintain elevated oxidative conditions, an area being actively investigated in nutritional oncology research. Cancer cells are known to have elevated oxidative stress; pro-oxidant strategies are being investigated in nutritional oncology research for how they may interact with these cellular conditions, while normal cells tolerate the restriction through alternative protective pathways. Research demonstrates that targeting methionine metabolism with recombinant methioninase overcomes gemcitabine resistance in pancreatic cancer patient-derived models, and early clinical case reports show tumor reduction when combining oral methioninase, low-methionine diet, and chemotherapy.
Practical methionine restriction emphasizes:
- Plant-based proteins (legumes, vegetables) over animal proteins (meat, dairy, eggs) — reducing animal protein intake without causing malnutrition can support metabolic wellness, reduce IGF-1 levels, and is being explored alongside conventional care in ongoing research
- Fruits and vegetables as dietary staples
- Limited intake of nuts, seeds, and grains (higher methionine content)
- Cycled restriction periods alternating with normal eating to prevent malnutrition
This scientific rationale forms the basis of the NORI Protocol—a structured methionine-restriction approach combined with targeted nutraceuticals developed by the Nutritional Oncology Research Institute. NORI provides personalized protocols with ongoing support for patients worldwide, designed to integrate with or complement a patient's broader treatment plan.
Pancreatic Enzyme Replacement and Vitamin Supplementation
Most pancreatic cancer patients develop exocrine insufficiency, causing severe malabsorption of fats and fat-soluble vitamins (A, D, E, K). Without intervention, this leads to steatorrhea (fatty stools), progressive weight loss, and critical nutrient deficiencies.
Pancreatic enzyme replacement therapy (PERT) addresses this directly, using prescription enzymes (typically pancrelipase) taken with every meal and snack to restore digestive function. Dosing is individualized based on fat content and symptom response—working with a dietitian experienced in pancreatic disease is essential to get this right.
Fat-soluble vitamin monitoring and supplementation:
- Vitamin D: Critical for immune function and bone health; routinely deficient in pancreatic cancer patients
- Vitamin K: Essential for blood clotting; deficiency causes bleeding risk
- Vitamin E: Antioxidant function; deficiency causes neuropathy
- Vitamin A: Vision and immune function; deficiency impairs tissue repair
Blood testing should assess these levels every 3-6 months, with targeted supplementation adjusted accordingly.
The Danger of Restrictive Fad Diets
ESPEN guidelines explicitly recommend against dietary restrictions that limit energy intake in patients with or at risk of malnutrition. PanCAN warns that ketogenic diets pose high risk of weight loss for pancreatic cancer patients experiencing fat malabsorption—even with enzyme adjustments. While a 2026 phase II trial showed feasibility of medically supervised ketogenic diet with chemotherapy, it required strict medical monitoring and is not appropriate for self-implementation.
The practical reality of eating with pancreatic cancer:
- Small, frequent meals (5-6 per day) to maximize nutrient absorption
- High-calorie, nutrient-dense foods to combat cachexia
- Prioritize maintaining weight over restrictive dietary theories
- Individualized guidance from experienced dietitians trumps generic diet plans
Evidence-Based Natural Compounds with Anti-Pancreatic Cancer Properties
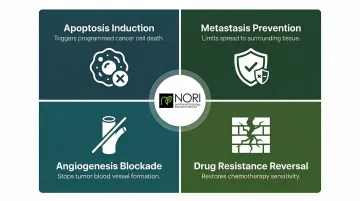
Traditional medicine systems—Traditional Chinese Medicine, Ayurveda, and Korean medicine—have contributed dozens of plant compounds now validated through scientific research. These natural products attack pancreatic cancer through several documented mechanisms:
- Cellular stress pathway modulation: being investigated for effects on cellular health in nutritional oncology research
- Metastasis prevention: limiting spread to surrounding tissue and organs
- Angiogenesis blockade: cutting off blood vessel formation that feeds tumors
- Drug resistance reversal: restoring sensitivity to chemotherapy drugs
Curcumin: The Most Studied Natural Compound
Curcumin, the active compound in turmeric, inhibits NF-κB—a master inflammation regulator overactive in pancreatic cancer cells. It demonstrates anti-inflammatory, pro-apoptotic, and anti-metastatic properties across multiple cancer types.
Clinical evidence: Curcumin has reached phase II clinical trials in pancreatic cancer patients, though standard oral curcumin at 8g/day yields poor plasma levels due to rapid metabolism. Nanoparticle formulations like Theracurmin safely achieve therapeutic blood concentrations without increasing chemotherapy adverse effects—making formulation critical to efficacy.
Plant-Derived Compounds with Strong Preclinical Evidence
Piperlongumine (from Piper longum): Sensitizes pancreatic cancer cells to gemcitabine by elevating reactive oxygen species, inducing cell cycle arrest, and inhibiting NF-κB activation. Animal studies demonstrate enhanced cellular health effects being investigated in research when combined with standard chemotherapy.
Moringa leaf extract: Aqueous extract down-regulates NF-κB, affects cellular stress pathways, and is being explored alongside conventional care in ongoing research (cisplatin/radiation) in pancreatic cancer cells. Additional research shows inhibition of tumor growth and metastasis in animal models.
Vitamin E delta-tocotrienol: Natural form of vitamin E that shows documented activity against pancreatic cancer stem cells—the highly resistant cell population responsible for treatment failure and recurrence. Has been investigated for its effects on cellular stress pathways through endoplasmic reticulum stress mechanisms.
Mistletoe extract (Viscum album): Despite widespread use in European integrative oncology, the 2024 MISTRAL phase III trial showed no overall survival or quality of life benefit when added to modern palliative chemotherapy. Patients currently using or considering mistletoe therapy should discuss these results with their oncologist before continuing.
Synergy with Conventional Drugs: Overcoming Resistance
Several natural compounds directly address chemotherapy resistance—one of the core reasons standard treatment fails in pancreatic cancer:
Coix seed extract: Synergistically enhances gemcitabine efficacy by downregulating drug efflux pumps (ABCB1 and ABCG2) that pump chemotherapy out of cancer cells, and by blocking NF-κB signaling that promotes resistance.
Bitter melon juice: Targets gemcitabine resistance by inhibiting PI3K/Akt signaling and specifically attacking pancreatic cancer stem cells—the treatment-resistant population responsible for recurrence.
Sodium selenite: Being studied for its role in cellular health pathways in nutritional oncology research, with over 40 years of research into its chemotherapeutic activity. Part of NORI's core nutraceutical protocol.
Important Caveats
Most evidence here is preclinical—cell culture and animal studies that human clinical trials haven't yet validated. Never self-prescribe high-dose supplements without guidance from an oncologist or integrative practitioner. Some compounds interfere with conventional treatments, alter drug metabolism, or produce unexpected side effects.
Work with a practitioner who understands drug-supplement interactions and can personalize a protocol to your specific cancer biology and treatment plan.
Mind-Body Practices, Lifestyle, and Emotional Support
The Psychological Burden: Why Mental Health Is Physiological
Pancreatic cancer patients exhibit the highest depression prevalence among major cancer types — estimates range from 33% to 50%. Cancer patients carry five-fold increased odds of depression compared to healthy individuals.
That burden isn't separate from physical health. Depression and anxiety directly affect treatment adherence, immune function, and inflammatory markers — meaning psychological support belongs in any serious treatment plan.
Gentle Exercise: Measurable Benefits Without Exhaustion
A randomized controlled trial of a home-based walking program in resected pancreas and periampullary cancer patients demonstrated improvements in fatigue (FACIT-Fatigue Scale), physical functioning, and health-related quality of life — starting slowly and building intensity based on individual tolerance.
Recommended low-impact activities:
- Gentle walking (10-15 minutes, gradually increasing)
- Yoga and stretching (modified for energy levels)
- Tai chi or qigong (mind-body integration)
- Light resistance training (preserves muscle mass during cachexia)
Key principle: Start at current capacity and build gradually. Exercise during treatment should enhance energy and reduce anxiety — not create additional stress or exhaustion.
Stress Reduction and Mental Health: Physiological Impact
A 2024 randomized controlled trial showed that mindfulness meditation significantly reduced anxiety, pain severity, and brain fatigue in pancreatic cancer patients undergoing chemotherapy, promoting overall quality of life. Mindfulness-Based Stress Reduction (MBSR) reduces salivary cortisol and pro-inflammatory cytokines (IL-6, TNFα) in cancer survivors — demonstrating measurable physiological changes, not just subjective mood improvement.

Evidence-based stress reduction practices:
- Mindfulness meditation (structured programs or apps)
- Support groups (peer connection reduces isolation)
- Cognitive-behavioral therapy (addresses anxiety and depression)
- Professional counseling (processes existential fears)
Sleep, Circadian Rhythm, and Environmental Toxin Reduction
The stress and cortisol dysregulation addressed above feeds directly into sleep disruption. Insomnia is highly prevalent following pancreaticoduodenectomy, compounding immune dysfunction and slowing recovery. Research on chronotherapy — timing chemotherapy to circadian rhythms — shows improved tolerability and response rates in GI cancers, underscoring how much biological timing matters.
Baseline lifestyle pillars:
- Prioritize 7-9 hours of sleep nightly
- Maintain consistent sleep-wake schedules
- Eliminate alcohol (increases cancer risk and worsens malnutrition)
- Avoid smoking and secondhand smoke exposure
- Reduce environmental toxin exposure where feasible
Taken together, these habits shape cortisol regulation, immune signaling, and how well the body tolerates treatment.
Integrating Holistic Approaches with Your Cancer Care Plan
The Multidisciplinary Team (MDT) Model
Optimal pancreatic cancer care requires coordination across specialties: surgical oncology, medical oncology, radiation oncology, pathology, radiology, genetics, dietitians, integrative practitioners, and mental health professionals. Evaluation at a Pancreas Multidisciplinary Clinic (PMDC) alters resectability assessments in up to 29.7% of cases.
Patients evaluated in a PMDC are twice as likely to complete recommended neoadjuvant therapy (treatment given before surgery), achieve better pathologic tumor responses, and undergo more R0 resections (complete tumor removal with clear margins) compared to those seen in individual specialty clinics. For patients, this means that where you receive care — and who coordinates it — directly affects your outcomes.

Building your MDT:
- Primary oncologist (coordinates conventional treatment)
- Surgeon specializing in pancreatic cancer (if surgical candidate)
- Dietitian experienced in pancreatic disease
- Integrative oncology practitioner (coordinates complementary approaches)
- Mental health professional (psychologist or counselor)
- Palliative care specialist (symptom management and quality of life)
Talking to Your Oncologist About Integrative Approaches
Effective communication about complementary strategies builds trust and prevents dangerous herb-drug interactions. Guidelines recommend exploring patient values, managing uncertainty, and guiding patients toward evidence-based therapies rather than dismissing integrative approaches outright.
How to approach the conversation:
- Use the term "integrative" rather than "alternative" (signals collaboration, not replacement)
- Bring peer-reviewed research articles, not testimonials or blog posts
- Ask specifically about potential interactions with your chemotherapy regimen
- Request referrals to integrative oncology practitioners if your oncologist is unfamiliar
- Emphasize your commitment to evidence-based approaches
Society for Integrative Oncology (SIO) and ASCO jointly recommend mindfulness-based interventions, yoga, and relaxation therapies for managing anxiety and depression, and acupuncture/acupressure for cancer pain management—providing oncologist-friendly guidelines you can reference.
Structured Nutritional Oncology Programs: The NORI Example
Once you've established open communication with your oncologist, structured nutritional programs offer a practical way to implement evidence-based complementary support. NORI (Nutritional Oncology Research Institute) offers personalized protocols combining cycled methionine restriction with targeted nutraceutical combinations — an approach built on founder Mark Simon's focused cancer research since 2004.
NORI's program works alongside conventional treatment or, for patients who have exhausted or declined conventional options, as a primary support approach. It's entirely home-based — no clinic visits required — with free initial consultations, unlimited ongoing support, and flat-fee monthly, yearly, or lifetime pricing.
Patients worldwide can reach NORI at 800-634-3804 or info@nutritionaloncology.net to discuss whether this structured approach fits their circumstances.
The Key Principle: Integration Requires Communication
Holistic treatment approaches deliver maximum benefit when they are evidence-informed, personalized, and implemented within a framework of open communication across your entire care team. The most effective strategy is one your full team knows about, supports, and can monitor — where conventional treatment and integrative support reinforce each other rather than operating in isolation.
Frequently Asked Questions
Can you survive stage 4 pancreatic cancer?
Stage IV pancreatic cancer carries a 3.2% five-year survival rate. Some patients do achieve longer survival through multimodal treatment combining surgery (when metastases are limited), chemotherapy regimens like FOLFIRINOX, and integrative nutritional strategies aimed at extending quality survival time.
What shrinks a pancreatic tumor?
Chemotherapy regimens (FOLFIRINOX, gemcitabine/nab-paclitaxel) and radiation therapy are the primary tools for shrinking pancreatic tumors, sometimes used as neoadjuvant treatment before surgery. Certain natural compounds (curcumin, plant extracts, vitamin E tocotrienols) have shown tumor-inhibiting effects in preclinical studies, though none replace standard treatment.
How to fight pancreatic cancer?
Fighting pancreatic cancer means working with a specialist multidisciplinary team to pursue all applicable conventional treatments — surgery, chemotherapy, and radiation — alongside evidence-based integrative strategies like dietary optimization and targeted supplementation under professional guidance. Maintaining weight through nutrient-dense eating and addressing mental health through counseling and support groups are equally important parts of a complete approach.
Is there a special diet for pancreatic cancer patients?
Pancreatic cancer patients generally do best with small, frequent meals, nutrient-dense whole foods, adequate healthy fats paired with enzyme replacement, and minimal refined sugar. Because roughly 72% develop exocrine insufficiency and severe malabsorption, individualized guidance from a dietitian experienced in pancreatic disease is strongly recommended over generic plans.
What natural supplements are used for pancreatic cancer?
The most studied compounds include curcumin (preferably high-bioavailability formulations), vitamin E tocotrienols (particularly delta-tocotrienol), sodium selenite, and plant-derived extracts (piperlongumine, coix seed, moringa). Supplementation should be guided by a qualified integrative practitioner to avoid interactions with conventional treatment and ensure appropriate dosing.
Can holistic treatments replace conventional pancreatic cancer treatment?
For most patients, holistic approaches work best alongside standard oncology care — improving treatment tolerance, quality of life, and overall outcomes. Integrative programs like NORI also support patients who have exhausted conventional options and are exploring nutritional and natural approaches under professional guidance. Any treatment decision should be made with full information and qualified support.