Introduction
Following an ovarian cancer diagnosis, many patients begin exploring options beyond the standard treatments of surgery and chemotherapy. Research shows this is far from uncommon: a 2017 UK study found that 25.1% of postmenopausal women reported using complementary or alternative medicine (CAM) therapies, while another study documented that 44% of ovarian cancer patients used CAM during chemotherapy.
Several factors drive this interest. Chemotherapy's severe side effects — nausea, fatigue, neuropathy — lead patients to seek supportive measures, while many want greater control over their treatment experience and quality of life. Others are focused on preventing recurrence, a real concern given that advanced ovarian cancer returns in over 80% of cases.
The search for integrative options that complement conventional care has become increasingly mainstream. Major cancer centers now offer evidence-based integrative oncology programs, reflecting a broader shift in how patients and clinicians approach the disease together.
This article examines what the evidence actually shows about natural and complementary approaches to ovarian cancer care, including nutritional strategies, plant-derived compounds, and mind-body therapies, with practical guidance on integrating them safely alongside medical treatment.
Key Takeaways
- Complementary therapies work alongside conventional treatment; alternative therapies replace it — a distinction that directly affects survival outcomes
- Plant-based diets and targeted nutrients show measurable effects on cancer cell metabolism and inflammation
- Quercetin, curcumin, and omega-3s show wellness-supporting activity in lab and animal studies — human trials are ongoing
- Acupuncture, yoga, and mindfulness effectively manage treatment side effects without interfering with conventional care
- Always disclose supplements and complementary approaches to your oncology team to prevent dangerous interactions
Complementary vs. Alternative Therapies: Why the Distinction Matters
The terms "complementary" and "alternative" are not interchangeable. Complementary therapies work alongside conventional ovarian cancer care—surgery, chemotherapy, targeted drugs—to manage symptoms, reduce side effects, and support overall wellbeing. Alternative therapies are used instead of conventional treatment.
This distinction has life-or-death implications. A 2018 study in the Journal of the National Cancer Institute found that patients who used alternative medicine in place of conventional treatment faced a 2.5x higher risk of death compared to those receiving standard care. Conversely, patients who integrate complementary approaches alongside conventional treatment often report improved quality of life and better treatment tolerability—without compromising survival.
Cancer care is shifting toward integration rather than opposition. Major centers now offer formal integrative oncology programs that combine natural treatments with standard care:
- Memorial Sloan Kettering — acupuncture, massage, and mind-body therapies alongside oncology treatment
- MD Anderson — nutrition counseling, meditation, and integrative consultations for cancer patients
- Mayo Clinic — evidence-based complementary care embedded within cancer care plans
For ovarian cancer patients, this means the choice isn't always between natural and conventional — it's increasingly about how to combine them effectively.
Nutrition and Diet as a Foundation for Ovarian Cancer Support
Dietary choices actively shape the metabolic environment that ovarian cancer cells depend on to grow. Ovarian cancer cells rely on specific pathways to fuel proliferation, and targeted nutrition can disrupt those pathways. Nutritional oncology — the science of using diet and targeted nutrient strategies — represents one of the most evidence-supported natural interventions available.
Dietary Patterns That Support Ovarian Cancer Recovery
Research consistently shows that predominantly plant-based diets rich in vegetables, fruits, legumes, and whole grains provide protective benefits. A 2026 review concluded that plant-based diets favorably influence ovarian cancer risk, while diets high in ultra-processed plant foods increase risk. These protective effects come from fiber, antioxidants, and anti-inflammatory phytochemicals that reduce systemic inflammation — a known driver of ovarian cancer progression.
The benefits are specific and measurable:
- Flavonoid-rich foods including apples, onions, tea, and citrus have been linked to reduced ovarian cancer risk in epidemiological studies
- Anti-inflammatory eating patterns contrast sharply with pro-inflammatory diets; research shows pro-inflammatory diets may increase ovarian cancer risk in postmenopausal women
- High-quality dietary patterns including the Healthy Eating Index 2020 show significant association with improved survival outcomes
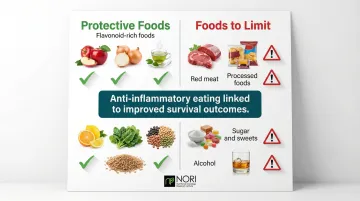
Foods to limit include added sugars, processed and red meats, and alcohol, all of which are linked to increased cancer risk and systemic inflammation.
Methionine Restriction: A Targeted Nutritional Strategy
Methionine restriction exploits a specific metabolic vulnerability in cancer cells. Methionine is an essential amino acid abundant in animal proteins, and cancer cells show a unique dependence on dietary methionine compared to normal cells (a phenomenon known as methionine dependence, or the Hoffman effect).
Research spanning decades has shown that most cancer cells cannot proliferate when methionine is restricted, leading to cell cycle arrest and programmed cell death. Normal cells can obtain methionine through alternative metabolic pathways. This makes dietary methionine restriction a selective strategy — one that targets cancer cells while leaving healthy tissue relatively unharmed.
Reducing animal protein intake without causing malnutrition can support metabolic wellness, reduce IGF-1 levels, and is being explored alongside conventional care in ongoing research — the core dietary rationale behind methionine restriction. The NORI Protocol — developed by the Nutritional Oncology Research Institute based on 20+ years of focused cancer research — builds on this science through cycled methionine restriction combined with pro-oxidant nutraceutical combinations being studied in nutritional oncology research. Patients interested in applying this structured approach can request a free initial consultation with NORI at 800-634-3804 to explore whether this strategy fits their situation.
Managing Nutrition During and After Treatment
Practical nutrition during chemotherapy requires balancing therapeutic goals with treatment tolerability:
- Maintain adequate protein to preserve muscle mass, even while managing nausea
- Stay well-hydrated to support kidney function and reduce toxicity
- Adjust for side effects using bland, easy-to-digest foods when taste changes and appetite loss occur
- Work with a qualified oncology dietitian who can tailor guidance to your specific treatment phase
After treatment, the same anti-inflammatory dietary foundation that supports recovery becomes the basis for long-term recurrence prevention — reinforcing why nutrition isn't a short-term intervention but an ongoing strategy.
Natural Compounds and Phytochemicals with Research Backing
Phytochemicals—bioactive compounds from plants—have generated a growing body of preclinical research in ovarian cancer. Several show meaningful wellness-supporting activity in laboratory and animal studies, and a handful have reached clinical trials.
Quercetin
Quercetin, a flavonoid found in apples, onions, tea, and citrus, represents one of the most extensively studied natural compounds for ovarian cancer. Research shows quercetin is being studied for its effects on cellular health in nutritional oncology research, including its role in cell cycle regulation, tumor invasion, migration, and its effects alongside cisplatin.
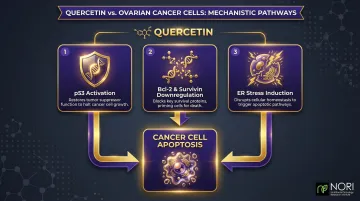
Key mechanisms driving these effects include:
- Activation of p53 (a key tumor suppressor protein)
- Downregulation of Bcl-2 and survivin (proteins that support cancer wellness cell death)
- Induction of endoplasmic reticulum (ER) stress, affecting cellular pathways, as investigated in nutritional oncology research
An active Phase 2 clinical trial at Memorial Sloan Kettering is investigating isoquercetin to reduce blood clot risk markers in ovarian cancer patients, demonstrating the compound's progression from laboratory to clinical application.
Most evidence remains preclinical, but the volume and reproducibility of findings support prioritizing quercetin-rich foods as part of a cancer-supportive diet.
Curcumin (Turmeric)
Curcumin, the active compound in turmeric, has demonstrated anti-inflammatory and anti-proliferative properties in multiple cancer types. A 2023 study found that curcumin and paclitaxel synergistically inhibited proliferation and promoted apoptosis in ovarian cancer cells, working through the miR-9-5p/BRCA1 pathway.
An important caveat: curcumin can interact with certain chemotherapy agents, potentially altering their effectiveness. Supplementation should only occur under medical supervision after discussion with your treating oncologist. Culinary use of turmeric in food poses minimal interaction risk.
Other Noteworthy Compounds
Green tea catechins (EGCG): Research shows EGCG inhibits ovarian cancer cell proliferation and invasion while reducing vascular endothelial growth factor, with clear anti-angiogenic activity. Evidence level: preclinical with promising mechanistic data.
Resveratrol: Studies demonstrate resveratrol induces autophagocytosis in ovarian cancer cells and inhibits glucose metabolism, a key cancer cell fuel source. Evidence level: primarily preclinical with interesting mechanistic findings.
Omega-3 fatty acids: Docosahexaenoic acid (DHA) significantly inhibited ovarian cancer cell proliferation and demonstrated wellness-supportingigenic activity in mouse models. Additionally, omega-3s may enhance chemotherapy response by targeting specific cancer cell pathways. Evidence level: strong preclinical data with some supportive clinical findings.
Mind-Body and Physical Complementary Therapies
For ovarian cancer patients managing chemotherapy side effects, post-surgical recovery, and ongoing anxiety, mind-body and physical therapies offer meaningful, evidence-backed relief — without disrupting standard treatment.
Acupuncture
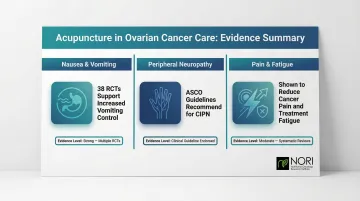
Clinical evidence supports acupuncture's role in ovarian cancer care for several specific applications:
- Chemotherapy-induced nausea and vomiting: A 2024 systematic review of 38 randomized controlled trials found acupuncture increased complete control of both acute and delayed vomiting when added to usual care
- Peripheral neuropathy: ASCO guidelines state acupuncture may be offered to patients experiencing chemotherapy-induced peripheral neuropathy
- Cancer pain and fatigue: Acupuncture shows benefit for general cancer pain, musculoskeletal pain, and treatment-related fatigue
Safety consideration: Western medical acupuncture uses sterile needles and is generally safe during treatment. However, patients on blood thinners or with low platelet counts should consult their care team first, as bleeding risk increases with very low platelets.
Mindfulness, Yoga, and Tai Chi
Movement and mindfulness practices complement acupuncture by targeting the psychological toll of treatment — anxiety, depression, and disrupted sleep — alongside physical symptoms like fatigue.
Research findings across these modalities:
- Yoga: A 2025 systematic review in gynecological cancers found meditative yoga reduced anxiety, depression, and stress while improving quality of life and fatigue. It also supports flexibility and muscle recovery post-surgery.
- Tai Chi: A 2026 meta-analysis found Tai Chi significantly improved cancer-related fatigue, making it especially useful for patients with balance issues or limited exercise capacity.
- Mindfulness meditation: Reduces anxiety and depression through structured stress-reduction practice. Even brief daily sessions show measurable benefit for treatment-related psychological distress in clinical studies.
Massage and Reflexology
Safety requirements to discuss with your care team before booking:
- Massage therapists must be trained specifically to work with cancer patients
- Deep tissue work may not be appropriate depending on tumor location, recent surgery, radiation sites, or implanted devices
- Patients with very low platelet counts (below 10,000) should avoid massage entirely due to bleeding risk
How to Safely Integrate Natural Approaches with Your Treatment Plan
The foundational rule: always disclose any complementary therapy, supplement, or dietary change to your oncology team.
Many natural compounds—particularly high-dose antioxidant supplements and herbal supplements—can interfere with chemotherapy or radiation by reducing the oxidative stress these treatments rely on to kill cancer cells.
Specific Supplements to Use with Caution
St. John's Wort: The most well-documented herb-drug interaction in oncology. It strongly induces the CYP3A4 enzyme and P-gp transporter, drastically lowering exposure to many anticancer drugs including docetaxel and irinotecan.
Garlic supplements and Ginkgo biloba: Both carry increased bleeding risk due to antiplatelet properties, which can worsen chemotherapy-induced low platelet counts.
High-dose vitamin C: While a Phase I/IIA trial found IV ascorbate reduced chemotherapy toxicities when combined with carboplatin and paclitaxel, preclinical data suggests high doses can interfere with doxorubicin and cisplatin cytotoxicity.
What a Good Integrative Care Conversation Looks Like
Knowing which supplements carry risks makes the conversation with your oncologist more productive. Bring a written list of anything you're considering and ask directly:
- Are there known interactions with my specific treatment regimen?
- Should timing be adjusted (for example, stopping supplements 48 hours before chemotherapy)?
- Can you refer me to an integrative oncologist or oncology dietitian?
If your current team isn't familiar with integrative oncology, ask for a referral — more oncology practices now include specialists in this area, and a single consultation can clarify what's safe for your specific regimen.
Red Flags That Signal Untrustworthiness
Avoid practitioners or therapies that:
- Claim a natural remedy can cure cancer without conventional treatment
- Request you keep the therapy secret from your medical team
- Pressure you to purchase expensive, unproven products
- Dismiss or denigrate conventional oncology
Any approach worth trusting will encourage open communication with your oncology team — not discourage it.
Frequently Asked Questions
Can ovarian cancer be treated without chemotherapy?
Surgery is the primary first-line treatment for many ovarian cancer stages. PARP inhibitors and targeted therapies are increasingly used as maintenance treatment. While some patients and researchers are exploring nutritional and integrative protocols, no natural approach has yet replaced chemotherapy as standard of care, though integrative methods can meaningfully support conventional treatment.
How to keep ovarian cancer from coming back?
Evidence-based recurrence prevention strategies include:
- Maintaining a healthy weight and anti-inflammatory, plant-rich diet
- Engaging in regular moderate exercise
- Adhering to prescribed maintenance therapies such as PARP inhibitors
- Exploring integrative nutritional protocols under professional guidance
What are the odds of ovarian cancer returning?
Recurrence occurs in roughly 25% of early-stage cases and over 80% of advanced-stage cases. Newer targeted therapies have improved recurrence-free survival, and nutritional and lifestyle interventions are increasingly studied for their impact on long-term outcomes.
Does ovarian cancer ever go into remission?
Yes, both partial and client-reported wellness improvements are possible, particularly after first-line surgery and chemotherapy. Ongoing maintenance therapy and supportive measures including nutrition and exercise can help extend remission periods.
Can ovarian cancer be cured completely?
Stage I ovarian cancer has a 92% five-year survival rate when caught and treated early. Advanced stages are more difficult to cure but can often be managed long-term as a chronic condition with the right combination of treatments and supportive care.
What are the new treatments for ovarian cancer?
Conventional advances include PARP inhibitors (olaparib, niraparib, rucaparib), mirvetuximab soravtansine-gynx approved in 2024 for platinum-resistant disease, and immunotherapy combinations. Nutritional protocols, nutraceuticals, and lifestyle-based therapies are also drawing increasing clinical interest as practical additions to standard care.


