
This article reviews the actual scientific evidence for natural treatments in rectal and colorectal cancer, covering herbal compounds, dietary strategies, and nutraceuticals—not as replacements for medical care, but as evidence-informed options worth discussing with your care team.
We'll explore natural compounds that have shown activity in lab and clinical studies, the role of diet and nutrition in cancer outcomes, and how an integrative framework can be built alongside standard treatment to maximize survival while maintaining quality of life.
Key Takeaways
- Natural treatments for rectal cancer have genuine scientific support — especially when combined with conventional care, not used to replace it
- Curcumin, green tea catechins, and omega-3 fatty acids show wellness-supporting activity in colorectal cancer research
- A fiber-rich, plant-forward diet low in processed foods and red meat reduces rectal cancer risk and improves treatment outcomes
- Correcting deficiencies in vitamin D, folate, and selenium can support immune function and treatment response
- Personalized nutritional protocols — tailoring diet and targeted supplements to the individual — offer the strongest integrative foundation
What the Research Actually Shows About Natural Treatments for Rectal Cancer
Not all natural treatments are created equal. Some show real biological activity against cancer cells in peer-reviewed studies; others are popular but lack clinical evidence. The research discussed here draws from the latter category — studies with measurable outcomes and published findings.
The Pine Street Clinic Survival Study
The strongest evidence for natural treatments comes from a landmark 10-year survival study published in Integrative Cancer Therapies (PMC4081504). Researchers followed 193 colon cancer patients who used a Pan-Asian medicine and vitamins protocol (PAM+V) alongside conventional therapy, comparing their outcomes to concurrent external controls from the California Cancer Registry and Kaiser Permanente.
The numbers tell a clear story:
| Cancer Stage | Hazard Ratio (HR) | 95% Confidence Interval | Control Group |
|---|---|---|---|
| Stage III | 0.71 | 0.51 - 0.98 | California Cancer Registry |
| Stage IV | 0.25 | 0.18 - 0.35 | California Cancer Registry |
| Stage IV | 0.25 | 0.19 - 0.34 | Kaiser Permanente |
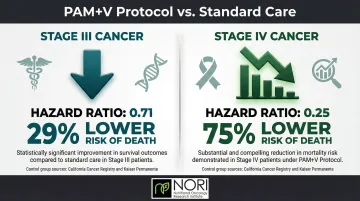
Patients with Stage III disease had a 29% lower risk of death, while Stage IV patients experienced a 75% reduction in mortality risk when combining PAM+V with conventional therapy.
Why Natural Compounds Are Biologically Plausible
Cancer cells have specific metabolic vulnerabilities that normal cells don't share. They depend heavily on certain amino acids like methionine, rely on aberrant signaling pathways like Stat3, and struggle to manage oxidative stress. Research shows that several plant-derived compounds exploit these vulnerabilities without harming healthy cells.
Research Limitations and the Integrative Model
Most compound-specific research comes from cell cultures or animal models. Few large randomized controlled trials exist for natural treatments in rectal cancer specifically. The Pine Street study, while promising, is observational and subject to selection bias—healthier or more motivated patients may have been more likely to pursue and maintain the protocol.
That said, even accounting for these limitations, research consistently shows that natural treatments perform best as a complement to conventional care. The strongest survival benefits appear in patients who combined both approaches rather than relying on either alone.
Natural Compounds with Evidence in Rectal and Colorectal Cancer
Curcumin
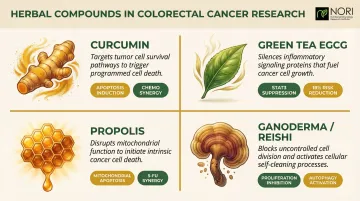
Curcumin, the active compound in turmeric, has been extensively studied in colorectal cancer research. Laboratory studies show it has been investigated for its effects on cellular stress pathways, is being researched for its role in metabolic health and cellular function, and is being explored alongside conventional care approaches in ongoing nutritional oncology research including 5-fluorouracil and oxaliplatin.
Research published in PubMed demonstrated that curcumin combined with FOLFOX (5-FU + oxaliplatin) produced significantly greater growth inhibition in HCT-116 and HT-29 colon cancer cells compared to either agent alone. The synergy operates by downregulating four key proteins that drive cancer cell survival: EGFR, HER-2, HER-3, and IGF-1R.
Clinically, a Phase IIa trial (CUFOX) confirmed that adding 2g/day of curcumin to FOLFOX chemotherapy is safe and tolerable in metastatic colorectal cancer patients, with improved survival signals.
One practical limitation: standard curcumin is poorly absorbed by the body. Advanced formulations — micellar vehicles (NovaSOL) or phospholipid complexes (Meriva) — significantly enhance absorption and are necessary to reach therapeutic tissue levels.
Cryptotanshinone and Herbal Extracts
Cryptotanshinone (CPT), isolated from Salvia miltiorrhiza (Danshen), inhibits the Stat3 protein that drives colorectal cancer cell growth and survival. In research supported by National Cancer Institute funding and published in Molecular and Cellular Biochemistry, CPT blocked uncontrolled cancer cell growth without harming normal cells in laboratory studies.
Other herbal compounds with research backing include:
- Green tea catechins (EGCG): Have been investigated for their effects on cellular stress pathways in colorectal cancer cells by downregulating STAT3 pathways. A meta-analysis showed reduced colorectal cancer risk associated with green tea intake (OR = 0.82).
- Propolis: Has been investigated for its effects on cellular health pathways through mitochondrial dysfunction in colon cancer cells and shows supportive activity when combined with 5-FU.
- Ganoderma lucidum (Reishi): Has been studied for its effects on cellular health in colorectal cancer cells including effects on cellular stress pathways and cell cycle, with metabolic wellness-supporting properties observed in animal models.
Omega-3 Fatty Acids and Fish Oil
Omega-3 fatty acids from fish oil suppress inflammation and inhibit colon tumor growth, including reducing excessive intestinal cell proliferation in high-risk individuals. In the EMT phase II trial, patients receiving 2g daily of EPA prior to liver resection for colorectal cancer metastases achieved meaningful overall survival benefits compared to placebo (HR for OS 0.40).
Omega-3 supplementation also featured as a core component of the Pine Street Foundation Protocol — a multi-agent nutritional intervention study that reported improved survival outcomes in advanced cancer patients.
Dietary and Nutritional Strategies for Rectal Cancer
Foods That May Reduce Risk and Support Recovery
A plant-rich, high-fiber diet has strong epidemiological backing for lowering colorectal cancer risk and improving patient outcomes. Cruciferous vegetables like broccoli, kale, and cabbage contain sulforaphane, which supports detoxification and cell-growth regulation. Berries and legumes provide fiber, resistant starch, and phytonutrients that feed protective gut bacteria.
Specific research findings:
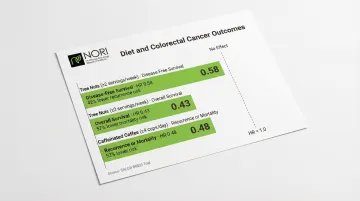
Tree nut consumption (≥2 servings per week) was associated with a 42% lower risk of disease recurrence in Stage III colon cancer patients from the CALGB 89803 trial. The same study found that consuming ≥4 cups of caffeinated coffee daily reduced cancer recurrence or mortality by 42%.
| Dietary Intervention | Intake Level | Hazard Ratio | Clinical Endpoint |
|---|---|---|---|
| Tree nuts | ≥2 servings/week | 0.58 | Disease-free survival |
| Tree nuts | ≥2 servings/week | 0.43 | Overall survival |
| Caffeinated coffee | ≥4 cups/day | 0.48 | Recurrence or mortality |
The Metabolic Angle: Methionine Restriction
Beyond specific foods, the composition of the overall diet shapes the metabolic environment that cancer cells depend on. Cancer cells rely heavily on methionine — an essential amino acid concentrated in animal proteins — and restricting it creates a vulnerability that healthy cells largely avoid.
Research published in Nature found that dietary methionine restriction disrupts one-carbon metabolism, exposing weaknesses in cancer cells' redox and nucleotide pathways. In colorectal cancer patient-derived xenografts, methionine restriction showed strong synergy with 5-FU chemotherapy, producing marked tumor growth inhibition.
NORI's protocol applies this finding directly: cycled methionine restriction combined with a targeted nutraceutical combination forms the core of their home-based nutritional support program, which has been used across colorectal and other cancer types. Patients interested in exploring this approach can reach NORI for a free initial consultation at 800-634-3804.
Foods to Reduce or Eliminate
Clear evidence points to specific dietary factors that increase colorectal cancer risk:
- Processed and red meats: The WHO/IARC classifies processed meat as carcinogenic (Group 1), with each 50g portion consumed daily increasing colorectal cancer risk by 18%
- Ultra-processed foods: Men in the highest fifth of UPF consumption had a 29% higher risk of developing colorectal cancer (HR 1.29) compared to the lowest fifth
- High-glycemic foods: Stage III colon cancer patients in the highest quintile of dietary glycemic load faced a 79% increased risk of recurrence or death (HR 1.79)
- Alcohol: Each 10g increase in daily alcohol consumption raises colorectal cancer risk by 7% (RR 1.07)
Integrating Natural Treatments with Conventional Rectal Cancer Care
Timing and Safety Considerations
Some natural compounds—particularly antioxidants—should be paused during certain phases of radiation and chemotherapy to avoid interfering with treatment. The Pine Street Protocol deliberately structured supplement use around the chemotherapy cycle: antioxidants were avoided during active chemotherapy days and resumed in the rebuilding phase between treatments.
This cyclical approach allows:
- Conventional treatments to work unimpeded
- Natural agents to support recovery during off-treatment periods
- Reduced side effects without compromising treatment efficacy
The Importance of Disclosure
Patients should inform their oncologist about all supplements and natural treatments, especially herbs with known drug interactions. Some compounds affect liver enzyme pathways that metabolize chemotherapy drugs. Working with an integrative-aware practitioner who can coordinate both approaches safely is the most practical solution.
Lifestyle Factors and Holistic Support
Research shows that lifestyle factors can directly influence cancer outcomes. Patients who incorporate the following alongside their treatment plan tend to report better quality of life and improved resilience:
- Physical activity: Even moderate exercise supports immune function and reduces fatigue during treatment
- Stress management: Practices like Qi Gong, yoga, and meditation help regulate the stress response, which affects inflammation and immune activity
- Emotional and mental health support: Documented integrative care plans for rectal cancer patients have combined naturopathic support with mental health interventions, with clinicians noting improved patient engagement and wellbeing throughout treatment
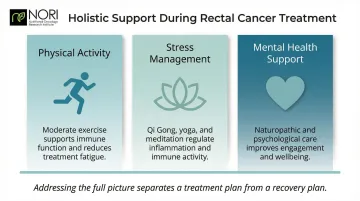
Addressing the full picture — not just the tumor — is what separates a treatment plan from a recovery plan.
Vitamin Deficiencies and Their Role in Rectal Cancer
Vitamin D
Low vitamin D levels have been associated with increased colorectal cancer risk and poorer outcomes in multiple studies. Vitamin D supports immune function, regulates cell growth, and promotes differentiation—functions that directly affect how cancer cells grow and respond to treatment.
Patients in treatment should have their vitamin D levels checked and corrected through supplementation if deficient. The Pine Street PAM+V protocol included vitamin D at doses ranging from 1,000–3,000 IU daily.
Folate (Vitamin B9)
Folate deficiency is linked to colorectal cancer risk because folate is essential for DNA methylation and repair. Deficiency raises mutation risk in rapidly dividing colorectal cells.
The PAM+V protocol specifically included folic acid supplementation at 400–1,000 mcg daily, recognizing its protective role in maintaining genomic stability.
Selenium and Magnesium
Both selenium and magnesium deficiencies are associated with increased colorectal cancer risk, though their mechanisms differ:
- Selenium supports antioxidant defenses through glutathione peroxidase, an enzyme that protects cells from oxidative damage. The Pine Street protocol included selenium at 100–400 mcg daily.
- Magnesium deficiency correlates with higher colorectal cancer incidence in epidemiological research. The exact mechanisms are still being studied, but correcting low magnesium levels is a reasonable step during treatment.
Testing for these deficiencies is straightforward, and targeted supplementation is low-risk when guided by lab results.
Frequently Asked Questions
Can rectal cancer be cured?
Rectal cancer, especially when caught early, has high survival rates with conventional treatment. Localized disease has a 90% five-year survival rate according to SEER data. Even advanced stages can achieve client-reported wellness improvements or long-term management with combined approaches that integrate conventional and natural therapies.
Can stage 4 rectal cancer achieve wellness improvements?
Stage 4 cancer wellness improvement is possible but less common than earlier stages. The PAM+V survival study found integrative approaches combining conventional and natural therapies were associated with positive wellness outcomes in observational research for stage IV colorectal cancer patients. Outcomes depend heavily on individualized care and close monitoring.
How can the growth of rectal cancer be stopped or slowed?
Several approaches can slow or stop rectal cancer growth:
- Conventional treatment: surgery, chemotherapy, radiation
- Dietary changes: low-glycemic, high-fiber, reduced processed foods
- Natural compounds: curcumin, omega-3s, green tea
- Metabolic targeting: methionine restriction to cut off a key cancer fuel source
How fast does rectal cancer grow and spread?
Rectal cancer typically develops slowly from polyps over years, but once established, growth rate varies by stage and subtype. Early detection via colonoscopy allows intervention before spread to lymph nodes or distant organs, which is why regular screening matters for everyone over 45, especially those with risk factors.
What is the survival rate for rectal cancer?
According to SEER data (2014–2020), five-year relative survival rates are 90% for localized disease, 74% for regional spread, and 18% for distant metastases. Research on integrative protocols has shown meaningfully better survival in advanced stages compared to standard care alone.
Are any vitamin deficiencies linked to rectal cancer?
Yes. Vitamin D, folate (B9), and selenium are the most researched deficiencies linked to increased colorectal cancer risk. Correcting these deficiencies may support immune function and improve treatment outcomes.
For patients interested in exploring evidence-based natural treatments alongside conventional care, NORI offers a free initial consultation to review nutritional protocols suited to your diagnosis and stage. Call 800-634-3804 or visit NORI's website to get started.


